![]()
PRN wishes you Gong Xi Raya
1996 - Something to chew on!
Dzulkifli Abdul Razak
If there is a word required to highlight major events in the year 1996, it would be 'food'. For it is during this year that a number of food-related incidences occurred - ranging from a world food summit to a massive food poisoning sending shock waves throughout the world; while at home, the cholera striked down more that a thousand victims nationwide. At the same time, what could be considered a new class of food appeared in the form of a genetically-engineered produce. In short, 1996 is a very 'foodful' year, providing us with lots to chew as food for thought for the coming years.
Incidentally, the year 1996 was also declared by the UN as the 'Year for the Eradication of Poverty'. Allegedly more than one billion people are living in absolute poverty, a problem no doubt is intractably linked to hunger, another of the world's scourge.
Hunger, like poverty is a tragic feature irrespective of time and place. It is not only confined to the South, notably Africa and south Asia; but is also present in the North among the OECD countries, especially implicating children. It has been said that more than half of the world goes to sleep hungry every night. To know that it exists in such a huge proportion really makes the stomach turn. Thus, when more than 7,000 delegates congregated in Rome for the World Food Summit, in November 1996, some guiding principles towards food security for all would have been discussed. The immediate aim is to halve the number of undernourished people from the present figure of over 800 million by 2015. At the end of it all, the Rome Declaration on food security was issued, signed and sealed. Some call it a farce. Meanwhile, in Ukraine for example, 126 people were killed and thousands others hospitalized after consuming poisonous mushrooms due to food shortage and the ironic prospect of a bumper harvest.
While the world continues to be concerned about poverty, malnutrition and hunger, seemingly as a result of shortage in food production, modern day practices of food production were being seriously scrutinized. It started in Europe where the public was stirred up by a food-related madness - bovine spongiform encephalopathy (BSE) or better known as the 'mad-cow' disease. Along with it came a new form of human disease, Creutzfeld-Jacob disease (CJD), which claimed more than 10 lives, thought to be linked to BSE. When the British government announced in March 1996 of the possibility of such a linkage, the sales of beef in Britain collapsed. British beef almost overnight was wiped of the menus the world over triggering numerous political, economic and social rows. The incident has raised yet another food-related controversy, namely the prevailing intensive farming methods that was adopted for years since the end of World War II. Organizations like the British Soil Association which promotes organic farming have been warning of the risks of such farming methods. For many, the negative effects of intensive farming have turned into a nightmare, and others predicted a change is imminent. Critics of modern farming continue to predict that this is just the latest string of disasters involving the food industry and is unlikely to be the last, unless food production practices are drastically reassessed.
As though to further drive the point home, two more 'mad-food' episodes emerged subsequently. These were the 'mad-sheep' scare - alleging that BSE has spread to sheep, forcing the US to put a ban on imports from Europe. Then there was the 'mad-beans' fatal episode in Nigeria, where so-called killer beans were being blamed for a series of sudden and mysterious death. Such a 'madness' comes close to summing up what the year is actually like.
Yet there was another aspect of modern practices in food production that drew global attention. This time it is the production of genetically-engineered soy bean which despite clearance by the US and EU health authorities raised a number of boycotts. They were protests in some 70 countries alleging that people using the produce could suffer allergic reactions, especially when used in infant formulae.
While hunger, poverty and 'mad-food' are making headlines across the world, so is the problem of food poisoning which under normal circumstances would be taken for granted. Although on many occasions food poisoning appears as a lesser evil, it nevertheless can be just as devilish. The year 1996 is indeed the case in point.
Internationally, the attack by a virulent strain of the E.coli, 0-157, on the Japanese population has for most part of the year kept every one alarmed and guessing. While the Japanese government warned its public not to eat raw meat; seafood and fruits were also in the suspected list of possible sources of the poisoning. The incident left about 10,000 people sick nationwide, about 200 mostly schoolchildren hospitalized, and more than 10 dead, making it the worst case in Japanese history.
Another global event of food poisoning that is not so well publicized took place in Scotland, also involving E. coli, but of a lesser strain. In any case, eleven died as a result. Ironically, the case is linked to meat pies supplied by an award-winning Scottish company in Lanarkshire. Yet another is in the U.S. where E. coli too caused the havoc. A study indicated that salami might be contaminated with the food-borne bacteria. More than 20,000 victims were reported each year, attributed to the lack of stringent food-processing safety standards. In fact, in US too, saw another outbreak of food-borne bacteria, salmonella, affecting more than 200,000 people. It was spread by ice-cream distributed from one of the states, Minnesota. The incident was said to be the largest cases of poisoning from a single source in the US. These examples however are but a small subset of a larger problem attributable to food poisoning reported in 1996. Other cases spanned the globe including those in Australia, Mongolia, India, Sri Lanka, Bangladesh, Hong Kong, China, Russia and of course Malaysia (see below) - just to name a few.
The impression left from these international events could best be described as 'schizophrenic'. While there are those who are starving to death in dire need for food, there are also those who are dying because of it. It seems that not only the system of food production and supply that needs to be addressed as purported in the World Food Summit in Rome, but equally important is the quality of food produced and supplied for human consumption. Otherwise more will be put at risk - with and without food.
Unfortunately, the scenario at the home front last year is not very much different. Although there are no abject poverty and starvation as depicted internationally, the year 1996 for Malaysia was equally 'foodful', albeit to a lesser extent. For a start, familiar questions regarding modern food production practices continued to be raised given the ample examples constantly reported in the local dailies. Apart from the regular issues of indiscriminate pesticide use, there was also a new outcry. The use of the antibiotic nitrofurans, in poultry feed became a national controversy. It got much attention after a survey carried out by the Health Ministry that showed far too much of the drug were found in poultry meat and eggs sold at the marketplace. In addition, there was also another concern namely the use of anabolic steroids to stimulate growth in pigs. Based on another survey, 90% of the pork sampled were reported to contain steroids. Also detected was a scheduled poison, a drug similar to beta-agonist.
All these seems to point out to the fact that in Malaysia practices of modern day food production too carry a certain amount of risk to the larger population. While the use of drugs and chemicals are accepted norms to maximize food yield, it can give raise to flagrant violation in the greed to generate quicker and fatter profits. In fact, in the case of the 'mad-cow' incidents, no one would have dreamt that cows, a plant-eating animal, would be fed with dead remains of sheep as part of intensive food production practices. Similarly the unscrupulous use of drugs like antibiotics or steroids is equally unthinkable in view of the undesirable health consequences that the public are exposed to. In the case of nitrofurans it was only after a disappointedly long hotly contested debates that the drug was banned from use in poultry feed. This is despite the worrying trend in antibiotic misuse nationwide.
There were many other less publicized food related incidences that also signal concerns, for example:
- seafood contaminated with cadmium in samples tested in Kelantan, Kedah and Perlis.
- high pesticide residues found in some vegetable produce sampled in Sabah.
- some samples of fishes (ikan kayu, ikan putih) taken in Sabah revealed to be contaminated with formaldehyde; similarly in Penang.
- sarer, a seaweed imported from Thailand was found to be contaminated with lead. It also contained high amounts of iodine and potassium, and was regarded unsafe even after cooking.
- some foodstalls in Penang were found to contain harmful colouring agents and contaminated with excessive coliform bacteria. One of the stalls was also selling belacan containing banned dye.
Such cases, seemingly isolated, provide a good spectrum of what could be only the tip of an iceberg.
One is tempted to arrive at this conclusion if reports on environmental pollution, especially of water sources are something to be taken seriously. For example in October alone, the following were recorded:
- The State Health Department in Malacca detected coliform bacteria in water supplied to about 2,500 families in 15 estates
- In Penang, the Department of Environment investigated illegal mud-dumping activities in the sea which have polluted the water and endangered at least 54 species of fish.
- In Penang too, Sungai Juru, once popularly used for cockle cultivation by the local population, was identified as the second most polluted river, after the infamous Sungai Pinang. Pig waste was the main source pollutant.
Indeed, in mid-1996, the 1995 Air and Water Quality Index revealed that agricultural activities, land clearing and discharge of industrial waste had worsened the water quality of rivers, notably in Perak. Ammonical nitrogen discharged by the rubber and latex-based factories were identified as the main pollutants of the rivers. Electroplating and textile industries were also implicated. And is most disheartening to note that barely a month into the new year, the death of an estimated 50,000 fishes - keli, lampan, putih - in Sungai Semberong, Kluang made the headline. Again pollution was implicated as the probable cause.
The event that took the cake was of course the cholera outbreak, another water-borne epidemic. Beginning from the island of Penang it slowly meanders into the other states as well, affecting more than 1,200 victims in all. Penang accounted for about 90% of the cases, making it the worst epidemic for the state in recent times. Some blamed weak physical infrastructure for the outbreak, but it is quite clear that 'care-free' attitude had a lot to do with it. At the heights of the outbreak many eatries, canteens and stalls had to be closed down because of failure to meet hygienic standards inspite of repeated reminders on the need to always keep clean. With such a prevailing attitude, it is not suprising therefore, the trend of food poisoning remained unabated over years. That schoolchildren are usually the main victims tell us that we may need to instill the right attitude at a very tender age.
In the light of all these developments, the Ministry of Health current 'Healthy Lifestyles Campaigns' focusing on eating habits must be taken seriously by all. The theme 'Healthy Eating' launched early this year is most appropriate in view of what 1996 has taught us. While Malaysia is blessed with the abundance of food, it is the quality that matters at the end of the day. The process of weaning away from the so-called affluent diets may not be a piece of cake, but it is a challange to be met.
However, not only should we be concerned about the affluent diet-related diseases - obesity, cardiovascular, diabetes - which is shown to be on the raise, but we must also seek ways to eliminate the most preventable of all daily occurrences, namely food poisoning. We need to at once rekindle the theme of the previous 'Healthy Lifestyles Campaigns' on food hygiene. In both cases what is required is the heightened and sustained awareness as to what we are putting into our mouth. After all as the saying goes, 'we are what we eat'. Of the two, food poisoning is much easier to avoid because it borders on good cultural habits and values. They are by and large common-sense and very few are in fact new or to be relearned anew. Hence in operational terms, the key recipe is not so much of what we know, but what we do with what we know in trying to inculcate good eating habits. Like they say the test in the pudding is to eat it!
In conclusion, it looks like the problem facing us is at least two-fold. While the lack of food is clearly a pressing problem, having food too could trigger equal concern. And as 1996 tells us, like food shortages, food-related diseases, especially poisoning, can transcend boundaries as well. That food poisoning is such a frequent occurrence worldwide is no wonder since according WHO, even in industrialized countries outbreaks of food-borne disease have been linked with inadequate cooking or re-heating, the use of contaminated ingredients and unsafe water, the preparation of food too far advance and its storage at room temperature, as well as cross-contamination between raw and prepared food. In fact diseases like cholera is fast re-emerging with some 384,403 cases reported in 1994 worldwide, a whooping 454 per cent increase from 1990.
In short, to have food is only part of the menu of solutions; what is important is the quality of the highest standard. In this regard, everyone in the food chain has an important role to play in safeguarding the standards of food quality. Like all approach to quality it begins with the mind - indeed a good food for thought.
Moving into its second year of operation, PRN has made some significant progress as shown by the list of Performance Indicators below. These indicators are specially designed as a measure to some of the major activities carried out by the centre. Details of the activities are documented separately and kept in the centre.
| PRN Report Card 1995-96 | |||
|---|---|---|---|
| Performance Indicators | 1995 | 1996 | % change |
| Overall Inquiries | |||
| 1087 | 1278 | +17.3 | |
| Acute Poisoning/Emergency Cases | |||
| 91 | 119 | +30.8 | |
| Laboratory Analysis | |||
| 5 | 435 | +8600 | |
| Consultancy/Research(completed) | |||
| 1 | 1 | - | |
| Bulletins (PRN8099/PenawaRacun) | |||
| 10 | 12 | +20 | |
| Published Articles/Book | |||
| 81 | 133/1 | +64.2 | |
| Papers Presented (International) | |||
| 33(1) | 78(4) | +136.4 | |
| Press Releases & Reports | |||
| 65 | 63 | -3.2 | |
| Radio & TV Programs | |||
| 10 | 28 | +180 | |
| Other Field Activities | |||
| 1 | 6 | +500 | |
| Post-graduate Supervision | |||
| 1 | 1 | - | |
| Number of Trainees (International) | |||
| 3(3) | 13(9) | +333.3 | |
| Continuing Education Enrolment | |||
| 50 | 97 | +94 | |
| Number of Visitors | |||
| 76 | 240 | +215.8 | |
| Seminars Organised | |||
| 1 | 3 | +200 | |
| Copyright (C) Pusat Racun Negara 1997 | |||
PRN CONSULT 
Review of CYCLIC ANTIDEPRESSANTS Overdose
Rahmat Awang, PharmD
Introduction
Cyclic antidepressants are among the most widely prescribed drugs for the treatment of depression in adults. Overdoses involving these drugs particularly among depressed patients occur quite frequently since many of them are very much prone to suicide. These drugs have low therapeutic index and overdoses have made it the leading cause of death in accidental and intentional drug overdoses. Seizures, hypotension, cardiac arrhythmias and respiratory depression which are considered life-threatening must be treated in the intensive care unit.
How many types of antidepressants are there?
In general, there are two major classes of antidepressants namely the monoamine oxidase inhibitors (MAOIs) and cyclic antidepressants. Among these, the cyclic antidepressants are the ones widely used. The MAOIs have a number of major drawbacks that limits their use. One is dietary restrictions and the other is drug-drug interactions; both having the potential of causing life-threatening hypertensive crisis.
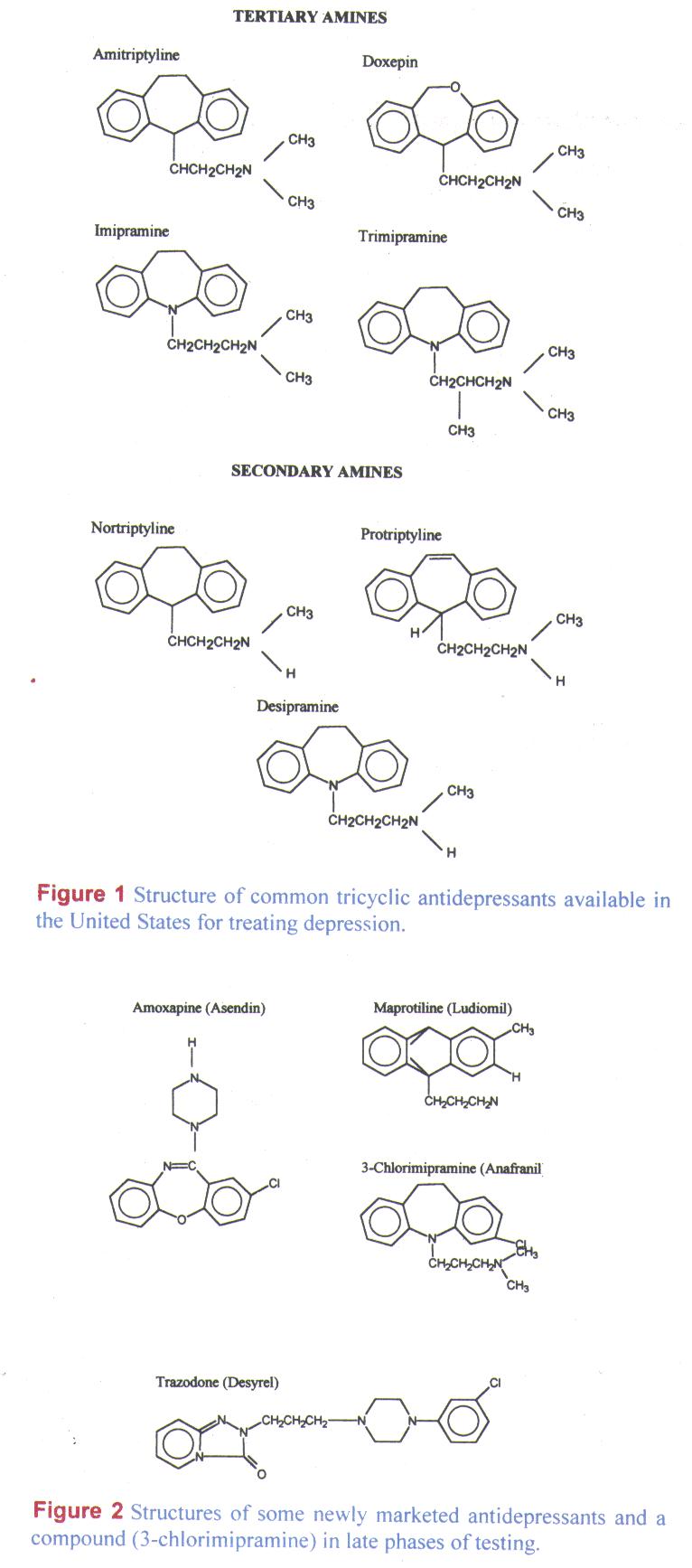
The cyclic antidepressants belong to a group of related compounds and they differ in their basic ring structure (see figure 1). The three-ring tertiary and secondary amines are the older cyclic antidepressants better known as tricyclics while the newer group comprises of one-, two-, and four-ring structures as well as the dibenzoxazepines. Tricyclic antidepressants (TCA) such as imipramine and amitriptyline are the protype tricyclic drugs while the newer types include maprotiline and mianserine (tetracyclic agents), amoxapine (dibenzoxazepine), fluoxetine (bicyclic) and vilozapine (unicyclic agents) and trazodone (triazolopyridine).
Which of these cyclic antidepressants are available in Malaysia?
Table 1 Cyclic Antidepressants Available in Malaysia
| Active Substance | Trade name, Dosage Form, (Strength), Manufacturer (Distributor) |
|---|---|
| Amitriptyline | Apo-Amitriptyline tablet (10mg, 25mg), Apotex Saroten tablet (10mg, 25mg), Lundbeck (Schmidt Scientific) Saroten Retard tablet (25mg), Lundbeck (Schmidt Scientific) Tripta tablet (10mg, 25mg, 50mg), Atlantic Tryptanol tablet (10mg, 25mg), Merck Sharp & Dohme (Summit) |
| Clomipramine | Anafranil tablet (25mg), Ciba (Ciba-Geigy[WM], Zuellig[EM]) Apo-Imipramine tablet (25mg), Apotex |
| Imipramine | Tofranil tablet (25mg), Ciba (Ciba-Geigy[WM], Zuellig[EM]) |
| Maprotiline | Ludiomil tablet (25mg, 50mg), Ciba (Ciba-Geigy[WM], Zuellig[EM]) |
| Mianserin | Remedica tablet (10mg, 30mg), Remedica (Waleta) Tovlon tablet (10mg, 30mg), Organon |
| Nortriptyline | Nortrilen tablet (10mg, 25mg), Lundbeck (Schmidt Scientific) |
| Trimipramine | Apo-Trimip tablet (25mg), Apotex (Waleta) |
WM - West Malaysia; EM - East Malaysia
How is cyclic antidepressants handled by the body?
When given in the usual therapeutic doses, cyclic antidepressants are well absorbed from the gastrointestinal tract. However in overdose condition, the absorption is slow with peak plasma concentrations achieved at up to 12 hours. This delayed absorption is a result of slowed dissolution and gastric emptying coupled with poor absorption when it become ionized in the stomach. In the blood, it is bound to a great extend to both body tissues and plasma proteins. The tissue uptake is rapid and results in high levels of the drug in the myocardium and the brain. The drug is metabolised in the liver and several active and inactive metabolites are produced in the process with some contributing to both the therapeutic and toxic effects of the agent (see table 2). With the cyclic antidepressants, enterohepatic recycling and modest excretion into gastric fluid and urine can also occur.
Table 2 Pharmacokinetic properties of selected cyclic antidepressants
| Drug | Bioavailability % | Protein Binding % | Volume of Distribution (L/kg) | Plasma Half-life(hour) | Active Metabolites |
|---|---|---|---|---|---|
| Amitriptyline | 31-61 | 82-96 | 5-10 | 31-46 | Nortriptyline |
| Clomipramine | NA | NA | 7-20 | 14-62 | Desmethyl derivative |
| Imipramie | 29-77 | 76-95 | 15-30 | 9-24 | Desipramine |
| Nortriptyline | 32-79 | 93-95 | 21-57 | 18-93 | 10-hydroxy derivative |
| Maprotiline | 66-75 | 88 | 15-28 | 21-52 | Desmethyl derivative |
| Mianserin | 30 | 90 | 47 | 10-17 | NA |
NA - Data not available
What are the pharmacological properties of cyclic antidepressants? What effects does it have in overdose?
Cyclic antidepressants possess a number of pharmacologic activities. They inhibit the reuptake of biogenic amines, both centrally and peripherally; block both the - and the acetylcholine receptors as well as possess quinidine-like or membrane-stabilizing local anesthetic effect on the heart. In overdose situation, the toxic symptoms may result from a combination of these actions.
Table 3 Effects seen from the pharmacological actions of cyclic antidepressants
| Action | Effects |
|---|---|
| Blockade of noradrenaline uptake at the synapses, centrally and peripherally | Transient hyperadrenergic state resulting hypertension, tachycardia and tremors. This is followed by catecholamine depletion which can result in hypotension. |
| Blockade of peripheral-receptor | Hypotension and reflex tachycardia. The degree of hypotension would probably reflect the critical nature of the patient. |
| Blockade of acetylcholine receptors, both centrally and peripherally | Sinus tachycardia (prominent but are usually not dangerous), agitation, seizures, coma, hallucinations and respiratory depression. |
| Membrane-stabilizing action | Conduction defects and arrhythmias with the following observations:
|
Clinically, the toxicity symptoms are presented with effects from central nervous system, cardiovascular and anticholinergic involvements.
The most common initial symptoms are related to the anticholinergic effects of the drug. These include mydriasis, tachycardia, dry mucous membranes, urinary retention, and decreased bowel activity. Confusion, agitation, and hallucinations can occur if the patient is awake. Twitching, jerking, and myoclonic movements have also been observed. Grand mal seizures take place in 11-20% of patients. Nystagmus, ataxia and dysarthria occur less commonly but occur early before coma precede. Respiratory depression is common due to the combined effects of anticholinergic activity and central sympathetic inhibition, and may lead to death in the absence of support. Progression to lethargy, coma and even ventillatory failure can occur very rapidly. The acidosis that often accompanies seizures may aggravate cardiotoxicity of antidepressants, possibly by increasing sodium channel inhibition. Hypoxia resulting from seizures may also aggravate cardiotoxicity. The cardiotoxic effects of cyclic antidepressants overdose include hypotension, cardiac arrhythmias and pulmonary edema. Severe hypotension or cardiac dysrhythmias has been the leading cause of death in cyclic antidepressant overdose.
Sinus tachycardia, being one of the most sensitive signs of cyclic antidepressant overdose is seen very early following the ingestion when anticholinergic symptoms predominate. Bradycardia, advanced heart block, asystole, supraventricular tachycardia, torsades de pointes, and ventricular fibrillation can also be encountered. Electrocardiographic changes and cardiac arrhythmias may be seen on arrival or develop within the first 2-6 hours after arrival. The severity of toxicity correlates with a QRS interval above 100msec and heart rate above 120, and a terminal 40 msec QRS axis greater than 120 degrees.
Among the cyclic antidepressants, the TCA has the greatest cardiotoxicity and anticholinergic side-effects. The newer antidepressants generally have similar toxicity after overdose to that of the original tricyclic antidepressants, although trazodone is less toxic. Maprotiline, when taken in overdose, cause more serious CNS adverse effects than the standard tricyclics. Acute renal failure and increased mortality are associated with amoxapine overdose. Although amoxapine does not cause the typical cardiovascular toxic effects of standard tricyclics, it produces a higher frequency of serious seizures, renal failure including rhabdomyolysis and acute tubular necrosis, coma, major irreversible neurologic sequelae, and greater risk of fatality. A high frequency of seizures may occur without corresponding cardiotoxicity or high mortality with the tetracyclic antidepressant (maprotiline) and the dibenzoxazepine (amoxapine). Second-generation antidepressants such as fluoxetine have minimal cardiovascular and anticholinergic toxicities.
At what dose has toxicity developed in cyclic antidepressant overdose and what is the prognosis?
Most cyclic antidepressants have a narrow therapeutic index. Thus, doses less than 10 times the therapeutic daily dose may produce severe intoxication. In adults, significant toxicity has been associated with doses ranging from 500 to 1000mg and ingestion of between 10 to 20 mg/kg is said to be potentially lethal. This however is only a general rule. As with all agents, there is wide variability in these estimations, and the degree of intoxication should be assessed based on individual signs and symptoms. In predicting the severity of overdose response it should be remembered that the severity is closely related to the patient's tolerance and that the assessment of the patient should be based largely on the clinical picture, more so than the amount ingested. Even then, the clinical pictures can change drastically in a matter of a few hours making it difficult to accurately predict the severity of the overdose.
In severe cases, patient may die during this first 24-hour and this is usually due to brain damage, respiratory problems, sepsis or multiple organ failure. Patients who survive this phase will have rapid and often dramatic recovery. Improvement in the level of unconsciousness may be seen within 12 hours with consciousness returning within 36 hours. Cardiac conduction defects and arrhythmias usually resolve within 12 hours but delirium and hallucinations may continue for up to 2-3 days or even longer.
When should one suspect cyclic antidepressant overdose and how can this be confirmed?
A patient with a history of depression and suicidal tendency that presents with lethargy, coma or seizures accompanied by QRS interval prolongation should be suspected for cyclic antidepressant overdose. The exception to this would applies for some newer antidepressants such as amoxapine and fluoxetine where seizures and coma may occur with no widening of the QRS interval.
Plasma levels of some antidepressants can be measured but this cannot be carried out routinely in hospital laboratories. Knowledge of the levels is not important in emergency situation.
However, if measured, levels of 1mcg/ml (1000ng/ml) or greater, of the parent drug plus its metabolites are usually associated with serious poisoning such as seizures, respiratory depression, prolonged coma and cardiac arrhythmias. Otherwise, the clinical manifestations of the overdose and the widening of the QRS are reliable indicators of toxicity, with QRS interval prolongation greater than 0.12s in the limb lead suggestive of severe poisoning.
How is cyclic antidepressant overdose managed?
Immediate action - emergency and supportive measures
All patients with cyclic antidepressant overdose whether confirmed or suspected should be evaluated even if there are no clinical signs of overdose. The signs and symptoms of cyclic antidepressant overdose usually appear within the six- hour period and it can last for 24 hours. If they remained asymptomatic during this period and results of diagnostic studies are within normal limits, psychiatric evaluation may be undertaken.
All symptomatic patients should be decontaminated and monitoring of the ventilatory status and electrocardiographic changes should be carried out continuously particularly in the first six hours. Patients with any degree of respiratory acidosis should be intubated and mechanically ventilated. Respiratory arrest can occur abruptly and without warning. All potentially life-threatening abnormalities such as coma, seizures, hyperthermia, arrhythmias or hypotension should be treated at once.
Removal of the cyclic antidepressants from the body
In adults, gastric lavage may be carried out with a large-bore tube following intubation if large amount of the cyclic antidepressants have been ingested. Gastric lavage can remove up to 22% of the ingested dose, although the average amount removed is about 9%. Insertion of the tube must be done with care because it is not without its own complication. Seizures and cardiac arrest have been reported to happen.
Once gastric lavage has been carried out, activated charcoal and a cathartic may be given at a dose of 50-100 g. Activated charcoal or cathartic alone without gastric emptying have been reported to be successful in the management of most tricyclic poisonings that occured with the first hour.
Repeated oral activated charcoal has also been suggested but its effectivess is still doubtful. Syrup of ipecac should not be used because patient can develop seizures or even lose consciousness rapidly. This can increase the risk of aspiration pneumonitis.
Management of complications
Once the basic treatments of preventing absorption and correcting electrolyte and acid-base problems have been addressed, specific complications can be managed.
Hypotension may develop and should be corrected initially with intravenous saline fluids. Serum pH should be determined promptly. Transfusion of whole blood, up to 20ml/kg in the first 2 hours, may be necessary to maintain blood pressure. If the blood pressure remains low despite adequate fluid being given, a vasopressor such as dopamine or noradrenaline may be given. The beneficial effect of dopamine in circulatory shock in this setting may be decreased due to compromise of the endogenous stores of noradrenaline caused by tricyclic antidepressants.
Arrhythmia is another complication that requires immediate attention as it is the leading cause of death in cyclic antidepressants overdose. Supraventricular and ventricular tachyarrhythmias can be prevented by alkalinizing the blood with bicarbonate or hyperventilation to a pH of 7.5. Supraventricular tachyarrhythmias as well as widening of the QRS, ventricular arrhythmias, and bradyarrhythmias should be treated with supportive care and alkalinization of the blood. Uncontrolled ventricular fibrillation and tachycardia may be treated with lidocaine 1-1.5mg/kg bolus, followed by an infusion of 2-4mg/minute. At high doses however, it may potentiate the myocardial depression of cyclic antidepressant overdose. Class I antiarrhythmic drugs including procainamide, disopyramide and quinidine are contraindicated and should be avoided because their membrane-stabilizing effects may potentiate the antidepressant toxicity. Beta-blocking agents such as propranolol are also dangerous and should be administered with care because their myocardial contractility and condeuction effects may worsen hypotension and cardiac depression. Thus, their use should be limited to patients with cardiac arrest caused by ventricular tachycardia or ventricular fibrillation not responding to all other measures.
Because generalised seizures may be followed by cardiac arrhythmias or ventilatory failure, patients should be monitored and treated immediately. Diazepam 0.15mg/kg should be administered at 15 to 20 minutes intervals until seizures are controlled or a total dose of 30-40mg. Phenytoin or phenobarbital infusions should then be instituted to prevent further seizures. Seizures that are not controlled with the usual anticonvulsants should be managed with pancuronium in order to paralyse the patient. This will prevent hyperthermia that can cause further seizures and lactic acidosis which can worsen the toxic effects on the heart.
Antidotal therapy
Some authors have suggested the use of physostigmine to reverse hallucinations, seizures, and the cardiovascular effects of cyclic antidepressants. Physostigmine is a cholinesterase inhibitor that can cross the blood-brain barrier. When given, it can make delirious, hallucinating patients become rational and lucid, regain consciousness or reduce the depth of the coma and slow heart rate in a matter of 5 to 10 minutes. There is no evidence to suggest that it is more effective than supportive management in reversing cardiac toxicity.
The indication for use include the presence of one or more of the following symptoms: seizures, deep coma, severe agitation and hallucinations, hypertension and cardiac arrhythmias. The therapeutic effects of physostigmine however are transient, i.e. about 30 minutes and may require repeated boluses or continuous infusions. Repeated administration is risky since this has been reported to precipitate seizures, hypersalivation, bronchial secretions as well as cardiac problems including ventricular fibrillation, idioventricular rhythms, and asystole. Thus, the use of physostigmine as antidote for cyclic antidepressants overdose should be reserved as a last resort to treat complications uncontrolled by other therapy.
Increased elimination
Forced diuresis, hemodialysis and charcoal hemoperfusion are reported to be ineffective in removing tricyclic antidepressants because these drugs are highly bound to blood proteins, have very large volume of distribution and are mainly eliminated by the liver; with only a very small fraction being excreted unchanged in the urine.