![]()
BREAKING OUT OF THE FOOD 'POISONING' CHAIN
Dzulkifli Abdul Razak
Food-related poisoning can be described as a chain of events. It normally starts from a single source and tends to spread via the methods of food production, preparation, storage, distribution and lastly consumption. Perhaps the recent cholera panic is a case in point, coming allegedly from ice suppliers spreading eventually throughout the state of Penang, and finally the whole nation. In every one of this situation the challenge is to break out of the chain of events. Indeed this is easier said than done because the nature and incidence of poisoning can also be influenced by agricultural practices, food technology in industry and at home, as well as other ecological, environmental, socioeconomic and cultural practices.
If the outbreak of cholera cases is to be classified broadly under the category of food poisoning, then it must epitomise the ultimate in a series of food poisoning cases in the country in recent times. While there has been a number of food poisoning cases reported last year, none garnered the same severity and thus attention as the cholera outbreak. The last being the loh see fun incident in Perak in 1988 where 14 school children died.
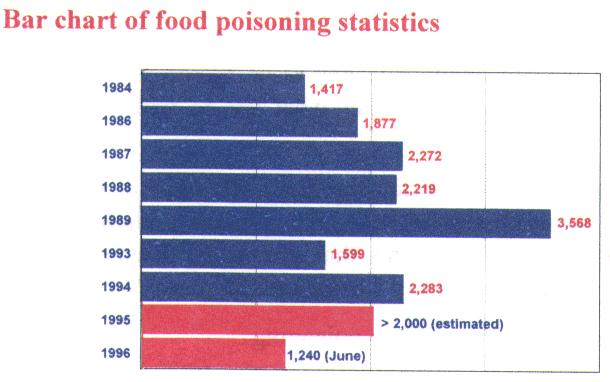
Nevertheless, as observed in PRN8099 (No. 6, Feb. 1996), food poisoning seems to be a recurring theme, and its occurrences are quite prevalent with a number of cases involving more than 100 victims, namely school children. In fact according to the Ministry of Health, generally there has been an increase in food poisoning cases from 1599 in 1993 to 2283 in 1994. And according to the same source, last year too there were more than 2,000 cases of food poisoning reported to the Health Ministry. Looking at the latest statistics for 1996, the cholera cases alone already amounted to more than a thousand cases nationwide. At the last count more than 1,240 cases were involved in practically all states. Although the situation is now well under control, there are still new cases being reported.
But this is not just the question of statistics, which no doubt suffers from under reporting. It is more the question of awareness and about Malaysians of all walks of life taking control on the situation in tandem with the national aspiration of a healthy society as enshrined in Vision 2020. The rather frequent cases of food-related poisoning, especially the like of cholera is most unfortunate. It is a chain that must be broken.
If we examine the literature, cases of cholera outbreak were mainly reported in countries that are rather backward in terms of health status. Even then, not all of such countries are faced with this predicament. By and large it has been well under control such that cholera vaccination is no longer a require-ment in many instances. In this context, for Malaysia, noted to its rapid development and infrastructure, to be faced with such an outbreak can be quite embarrassing. It is perhaps not so much the physical infrastructure that is at fault but rather own mindsets, worst still when it started in an urban centre like Penang. One would expect that most city dwellers by now should be knowledgeable enough about simple cases of food-borne diseases and how to avoid them. All that is required to stay free from food (water) borne illness like cholera, is to a large extent common-sense, most of which are being cul-turally advocated and practised. Very little in fact are new or need to be learned anew. The key issue therefore is not so much what we know, but rather what we do with what we know.
For example, most we are too familiar with some of the pre-cautionary actions listed below, which is really fundamental in preventing the chain of events that spread the disease in the first place. But are they being carried out diligently?
Precautions to avoid foodborne poisoning:
|
|
| Wash hands thoroughly before preparing, serving or eating food, especially after handling other things. | |
According to WHO, even in industrialised countries, out-breaks of foodborne disease have been linked with inadequate cooking or re-heating, the use of contaminated ingredients and unsafe water, the preparation of food too far advance and its storage at room temperature, as well as cross-contamination between raw and prepared food. As it stands to day, cholera is one of those so-called re-emerging diseases, with some 384,403 cases reported world-wide in 1994, a 454 per cent increase from 1990. So much so that WHO has created a new division to deal with such situations.
The Outlook for 1996
Apart from the cholera-caused food poisoning, there are a number of food poisoning cases being documented as of this month alone. Just when the incidences of cholera were peaking in mid-May, there was an equally disturbing report of bad chocolate-flavoured milk supplied to schools under the Education Ministry's school milk programme. Despite paying for the milk packets, sixty-one primary school children had fallen victim to what was described as a mild case of food poisoning. If not being overshadowed by the cholera cases, even such mild cases can be another embarrassing incident, because this not the first time it has been reported to happen. Moreover, it is an official programme of the government in the attempt to ensure the good health of pupils in schools. Ironically still, in this case the packets were reported to carry an expiry date of October 5, 1996 - some four months away. Something then must be amiss.
Going by the past records, the figures on food poisoning consistently show a worrying trend. Although the number is relatively reduced as compared to that of 1989, the recent cholera outbreak does seem to indicate that the situation is rather fragile, and schools are indeed vulnerable.
Taking just the schools and other educational institutions, there are about 10 incidences involving food poisoning since the beginning of this year. One involving as many as 400 victims, a couple more than 100 students, and in one school the incidence of food poisoning happened twice within the span of three months. If the number of cholera cases are taken into account, there must be almost 2000 known food-related poisoning cases even before we progress into the middle of 1996. Coupled this with the many recent initiatives taken by the appropriate agencies to educate hawkers and food-sellers about food safety in various states, including those in schools, we may still have a long way to go in combating food poisoning in our society.
The incidences involving schools are particularly of concerned because the issue about cleanliness of food operators in school canteens is indeed a contentious one. The Ministry of Education in particular has drawn up regulations to tackle this problem and periodic checks are supposed to be carried out. Despite all these the situation remains precarious, not least because in schools and educational institutions is where we should be teaching our children (and indeed teachers-to-be) about good eating habits in a practical way. In fact, the recent cholera outbreak started of with trainees in a teacher's training college. And according to the statement by the Minister of Health recently, of 3508 school canteens inspected in 1994, only 21 per cent were classified as clean, and the majority (72.3%) are moderately clean. Meaning to say that only a small proportion of our school children are relatively well protected from food poisoning chain of events. If this is so, there must be something more that need to be considered in our effort to improve the situation.
Food for Thought
School canteens and cafeteria, besides providing gastronomic supplements, should at the same time be feeding the minds as well, on matters related to food and associated activities. In other words, it is not just the question of cleanliness per se but more so the practice the goes along with it. While aspects of hygiene are taught, they must also be constantly re-enforced and demonstrated as well as performed daily. These should involve active learning and not just rules and regulations to be implemented during breaks or recess times. The whole process in fact is the introduction to, and cultivation of a new set of food-related habits. The school canteens and cafeteria can be regarded as an extension of the classroom where we instill the training of the minds of the pupils as far as these aspects are concerned. After all habits are acquired, and schools can be an effective place where the good ones are instilled, and the bad ones changed, if the right approach is adopted. This is what learning is all about, and failing to do so would meaning there will be greater risk to food poisoning in this case.
There is also the question of making the right choice. This is imperative because we are what to eat and making preferences for the type of food is again basically an acquired habit and perhaps a matter of fine-tuning the taste buds over a period of time. This aspect has been too much taken for granted by parents, pupils and teachers alike that some of the current menu does not seem to reflect a healthy lifestyle that we are insisting upon. For example the sugary menus (especially in drinks and some local kuih) as well as sweet-eating habits between meals have not be seriously dealt with. This is something that we ought to reconsider because excess in diet is the major cause of dental decay and also in the long run be a factor in many diseases. Thus concerted health education on sweets and sweet foods can lead to the formation of healthy habits that can complement the government's effort to combat diabetes for example. In fact a study looking at the prevalence of diabetes amongst Malays and aborigines in various socio-economic locations in Malaysia, showed the pevalent of diabetes was closely linked to overweight. Students therefore should be weaned away from the so-called affluent diet, a pattern of eating dominated by high consumption of energy-dense foods of animal origin and of foods processed or prepared with added fat, sugar and salt. In contrast, we need a reasonable diet, with plenty of vegetables and fruits.
Many research findings have confirmed the well-founded suspicion that dietary preferences may influence the onset of several major chronic diseases. Our scientific knowledge is adequate, and we have enough experts to assist us in formu-lating new strategies. In short, new nutritional goals and eating habits for school children must be established. Schools too should take appropriate actions based on best information cur-rently available on the effect of diet and health (see accompanying report).
Perhaps it is also timely for schools to dwell upon the notion that food can indeed affect mental performances. It has been shown that by taking the different combination of foods or at the wrong time can result in sluggish mental functions. It reflects not only the quality and quantity of food we eat, but also shows the extent our bodies can tranforms it to nutrients that will protect our health, both mentally and physically. Apart from the concept of balance diet, this aspect is indeed very relevant to the learning environment in schools and many are still quite oblivious to it.
Thus in captive situations where canteens and cafeteria are located, they should be playing a role of more than just trading posts but be exampleries as what good eateries should be like. They should also educate, other than just sell, so that pupils can begin to appreciate what they are putting in their mouths. It is pertinent that the children put their knowledge into practice. This mental training is all important because it will be the ultimate guiding principles in assisting them the moment they leave the school compounds. What the children have learned will remain school knowledge unless they are able to transfer it to their lives in some relevant and practical ways. More important still is when they are confronted with the many junk food promotions that are specifically targeted to children of all ages, not least via the TV network. Already the younger generations have the tendency to regard traditional food as outdated even if they are nutritious. Only when equipped with a strong educational foundation and understanding about the value of foods, can they make informed decisions and begin to discern which eateries should be patronised and which ones they should stay away from; equally important what food to buy and which one to avoid. It is only at this stage can we hope that incidences of food poisoning can be drastically reduced.
As it stands today, it is rather disheartening to see that there are still many who are patronising the hawkers and food stalls situated outside the school fences, especially after the schooling period (even at times of the cholera outbreak). Judging from such daily occurrences in many schools, pupils seem to prefer the menu presented by the hawkers. This is certainly not an offence, but by and large the quality of food and the way they are sold remain much to be desired by most standards. For example, in the 1994, of the 1517 hawkers inspected, almost 10 per cent were put in the poor and very poor categories compared to only 6.4 per cent were categorised as good. The rest are just average (64.1%). In matters concerning food, average may not be good enough because casually one can still see many food operators and sellers handling food and money alternately with the same bare hands. Thus introducing whatever contaminants from the latter to the former and passing them on to the consumers, each time exposing them to greater risk of food poisoning.
In Malaysia, hawkering is a way of life and we can be proud of it if only they sell good wholesome food based on hygienic practices. At the same time, there are many localised reasons for the emergence and re-emergence of diseases and food can be just another reason if we are not careful. In accepting these new reality, there is therefore an urgent need to teach all the potential consumers not to be so gullible such that they unknowingly are endangering their health. And the next best thing to do is to sensitise them with the correct attitudes and role models. What better way if not to start at the very early stage in their schooling life. In this context schools canteens and cafeteria at all institutions of learning have a vital role to play and should be geared up to meet this purpose as well. It may be our only hope to break out of the food poisoning chain.
| ASIAN CUISINE A RECIPE FOR HEALTH |
|---|
|
Rahmat Awang, PharmD
Introduction
Calcium channel blockers are widely used in the management of a variety of cardiovascular disorders including angina pectoris, hypertension and supraventricular tachyarrythmias and numerous other non-cardiovascular conditions like exercise-induced asthma and migraine headache. With increased used, there has been an increase in the number of overdose cases particularly with the three most readily available calcium channel blockers namely, verapamil, nifedipine and diltiazem.
The annual report published by the American Association of Poison Control Centers indicated an incidence in the reported cases of accidental and intentional overdoses from 96 in 1983 to 6,183 in 1992. Management of these patients presents a big challenge to the attending doctor because these drugs are quite toxic with the potential to cause serious morbidity and mortality while questions regarding the optimal therapy remain unresolved.
In this issue of PRN8099, we intend to discuss the toxicity that accompanies calcium channel blockers as well as the approach to managing these cases taking into consideration the various therapeutic modalities available.
What are the currently available calcium channel blockers in Malaysia and how do they differ in their pharmacologic properties?
Table 1 provides a list of calcium channel blockers that are available for use in Malaysia. They are a chemically heterogenous group of drugs. Verapamil, nifedipine, and diltiazem for example are chemically different with verapamil being a papaverine derivative, nifedipine a fat-soluble dihydropyridine derivative and diltiazem a benzothiazine derivative. Though their mode of action is similar, the pharmacological effects of these drugs may be different when given at therapeutic doses. All three drugs dilate blood vessels but this effect seems to be more pronounced with nifedipine compared to verapamil and diltiazem. The electrophysiological effects on the heart however is more pronounced with verapamil and diltiazem. Verapamil as such can exert a significant negative inotropic effect and usually has a profound effect on the AV node. The newly introduced calcium channel blockers including nicardipine, nimodipine, isradipine, felodipine and amlodipine have pharmacological properties closer to the nifedipine, having greater activity on the vascular smooth muscles. In overdose situation, these agents are expected to give similar effects to other agents in the class, except that they have less tendency to cause conduction defects compared to verapamil or diltiazem.
| GENERIC | TRADE NAME | GENERAL | PHARMACOLOGICAL PROPERTIES | |||
|---|---|---|---|---|---|---|
| CONTRACTILITY | HEART RATE | AV NODAL CONDUCTION | VASCULAR RESISTANCE | |||
| Amlodipine | Norvasc | Selective vascular actions | No effect | No effect | No effect | Decrease |
| Diltiazem | Cardil, Herbesser/ Herbesser 60,Herbesser Injection, Herbesser 90 SR, Tildiemr | Vascular and electrophysiologic actions | Decrease | Decrease | Decrease | Decrease |
| Felodipine | Plendil | Predominantly vascular actions | Minimal or no increase | Minimal or no increase | Minimal or no increase | Marked decrease |
| Flunarizine | Sibelium | Selective vascular actions | No effect | No effect | No effect | Decrease |
| Isradipine | Dynacirc/ Dynacirc SRO | Predominantly vascular actions | Minimal or no increase | Minimal or no increase | Minimal or no increase | Marked decrease |
| Nicardipine | Cardepine | Predominantly vascular actions | Minimal or no increase | Minimal or no increase | Minimal or no increase | Marked decrease |
| Nifedipine | Adalat, Adalat Retard/Adalat LA, Nifecard | Predominantly vascular actions | Minimal or no increase | Minimal or no increase | Minimal or no increase | Marked decrease |
| Nimodipine | Nimotop | Predominantly vascular actions | Minimal or no increase | Minimal or no increase | Minimal or no increase | Marked decrease |
| Verapamil | Isoptin | Vascular and electrophysiologic actions | Marked decrease | Decrease | Marked decrease | Decrease |
Should we be alarmed when somebody ingests an overdose of calcium channel blockers?
Calcium channel blockers have a relatively small toxic to therapeutic ratio. Toxicity may occur with administration of therapeutic doses and this is even more likely in patient who is also suffering from underlying hepatic or renal dysfunction or as a result of drug-drug interaction. Sensitivity to these agents can be modified by in the host disease particularly cardiovascular disorders. Concomittant use of some drugs like the beta blockers may increase the likelyhood of patients experiencing toxicity of calcium channel blocker at doses lower than usual.Doses greater than the usual recommended therapeutic range should be considered potentially life-threatening. Death have been reported for both verapamil and diltiazem at doses of 4.16 gm of immediate release and 7.2 to 9.6 gm of sustained release for verapamil preparations and between 0.7 to 2.88 gm of diltiazem. There has been no reported death case associated with nifedipine but an ingestion of about 50 mg was associated with signs of toxicity.
What are the signs and symptoms of calcium channel blocker poisoning?
Calcium channel blockers overdose may result in effects associated with cardiovascular, gastrointestinal, central nervous systems as well as glucose metabolism. Symptoms however depend on the amount, route and type of calcium channel blocker ingested. The classical presentation are hypotension and bradycardia.
Hypotension may be caused by peripheral vasodilation, reduced cardiac contractility, slowed heart rate, or a combination of all of these. Bradycardia may be due to sinus bradycardia, second or third degree atrioventricular block or sinus arrest with junctional escape rhythm. Calcium channel blockers do not affect intraventricular conduction, so the QRS duration is usually not affected. The PR interval is prolonged even with therapeutic doses of verapamil.
Overdose involving nifedipine usually presents with hypotension which may be accompanied by cardiogenic shock and idioventricular rhythms. This is particularly likely to occur in patients with underlying cardiovascular disease. With verapamil, hypotension and bradyarrythmias (especially in the form of junctional escape rhythm due to sinus bradycardia or atrioventricular block) are the most common manifestations.
Patients with massive overdoses may also present with slow idioventricular rhythms and prolonged QRS intervals. The features of acute diltiazem overdosage are similar to those of verapamil with hypotension and dysrhythmias, both occuring at equal frequency except verapamil is associated with a lot more conduction problems. Death and life-threatening complications such as heart block and refractory hypotension, are much more common with verapamil than diltiazem. Similarly, these effects are more common with diltiazem than nifedipine.
Table below provides a comparative summary of the toxic effects of these three drugs as reported by Ramoska et. al: A one-year evaluation of calcium channel blocker overdoses - toxicity and treatment (Annals of Emergency Medicine Vol. 22, Number 2 February 1993.
| EFFECTS | NO. OF PATIENTS | ||
|---|---|---|---|
| VERAPAMIL | NIFEDIPINE | DILTIAZEM | |
Hypotension
|
20 7 27 (53) |
9 0 9 (32) |
11 2 13 (38) |
Sinoatrial Node Depression
|
9 6 15 (29) |
4 0 4 (14) |
7 3 10 (29) |
Atrioventricular Node Depression
|
14 7 5 2 28 (55) |
1 1 0 3 5 (18) |
4 2 0 4 10 (29) |
Dysrhythmias
|
12 2 9 6 29 (57) |
16 0 0 0 16 (57) |
9 1 3 2 15 (44) |
| Total | 51 | 28 | 34 |
The overdosed patient may also develop non-specific symp-toms of nausea, vomiting, headache and lightheadedness. Central nervous system involvement including seizures and altered mental states such as stupor confusion, and coma have also been reported; believed to be due to reduced cardiac output and decreased cerebral perfusion. In addition to these, hyperglycemia and metabolic acidosis have also occurred.
How soon would we be able to see toxic signs of calcium channel blocker overdose?
The effects are often precipitous. Deterioration of vital signs are often sudden and profound. Symptoms usually develop within 30 to 60 minutes of ingestion of an overdose of five to 10 times the therapeutic dose. The symptoms however may be delayed up to greater than 12 hours from the time of ingestion with the sustained release preparations or immediately follow-ing intravenous administration. Recurrent toxicity after 24 hours has also been reported and patients who respond to ini-tial treatment frequently experience subsequent deterioration.
How do you explain the toxic manifestations observed with calcium channel blocker overdose?
Calcium is a cation that plays a key role in the regulation of cellular movement and transport, electrical activation of excitable cells and different enzymatic enzymes. The move-ment of this cation from the extracellular space to the intracellular space is governed by three types of calcium channels, namely, the receptor-operated calcium channels, stretch-operated calcium channels, and the voltage-sensitive calcium channels. The voltage-sensitive calcium channels can be classified further based on their conductivities and sensiti-vities to voltages into the L, N and T subtypes. Many of the physiological effects observed from the use of calcium channel blocker is a consequence of its action on the L channels. Inhibition on the receptor-operated channels have also been reported but the clinical significance of this effect is uncertain.
As a class, calcium channel blocker slows down the influx of calcium through the cellular calcium channels in the myo-cardium and vascular smooth muscles causing reduction of the electromechanical contraction in the atrial and ventricular muscle cells, slowed pacemaker activity in the SA and the AV node, reduced AV conduction, and vasodilatation of smooth muscle cells. The effect however depends on the type of calcium channel blocker as well as the concen-tration. Vasodilatation result in hypotension, flushing and headache while myocardial depression has resulted in hypotension, congestive failure, or frank cardiogenic shock. Central nervous system involvement is believed to be due to reduced cardiac output and decreased cerebral perfusion while the hyperglycemia which is commonly seen in verapamil and diltiazem overdose cases is probably related to blocking cal-cium entry into pancreatic islet beta cells, resulting in impair-ment of insulin release.
How can the overdosage be confirmed and what laboratory tests are usually carried out?
Good history taking and strong clinical suspicion are the only immediate modalities available. Any patient who present with hypotension and bradycardia, particularly with sinus arrest or AV block, in the absence of QRS interval prolongation should be suspected of having ingested these drugs. The differential diagnosis should include beta blockers and other sympatholytic drugs. CBC, electrolytes, glucose, BUN, creatinine, arterial blood gases, ECG and electrocardiographic monitoring.
Some authors believed that the clinical effects correlate with the drug's concentration and advocate the measurement of the drug's concentration. This idea however is debatable because the clinical outcome from an overdose do not correlate well with the drug's concentration. Generally, it is felt that there is little value in performing the measurement routinely since it does not predict toxicity and that it does not determine the way the patient is going to be treated. Moreover, it can only be carried out in specialised centres and the cost would be substantial.
What is the usual approach of managing calcium channel blocker overdose?
The treatment of calcium channel blocker overdose is largely supportive. The patient's airway should be maintained while coma, hypotension, and bradyarrythmias should be treated when they occur. Clinical status of the overdosed patient have been reported to change abruptly. The vital signs and electrocardiogram should be monitored at least for 24 hours even if the patient is not symptomatic.
Within the first few hours following ingestion, steps must be taken to remove and reduce absorption of the calcium channel blockers involved from the gut. Inducing emesis with syrup of ipecac should be avoided since the overdosed patient may at anytime develop CNS depression, seizures, hypotension or cardiac arrhythmias. Moreover, emesis may cause stimulation of the vagal nerves and this may worsen any pre-existing cardiac arrhythmias. Lavage should be carried out as soon as possible using a large bore orogastric tube to decrease absorption of the drug. This may be followed by administration of activated charcoal and a saline cathartic or sorbitol. If a sustained release preparation is involved, repeated doses of activated charcoal may be administered. Alternatively, whole bowel lavage using polyethylene glycol may be used in patient that has ingested a sustained release preparations. This is felt to be more effective than charcoal with an osmotic cathartic and has the advantage of not causing intravascular volume depletion.
Hypotension should be treated initially with intravenous normal saline. Most patients may not respond adequately to intravenous fluids alone if the hypotension is due to impaired myocardial contractility. In these cases, intravenous calcium may be given as the initial drug therapy. Calcium have been reported to improve conduction abnormalities, cardiac contractility and hypotension. The results have been mixed, some with clinical success while others have failed to show clinical improvements with doses as high as 24,000 mg (108 mEq) over 44 hours. The rational for therapy is to overcome a competitive blockade of calcium channels in the cardiac conducting system. The optimal dose required for this purpose has not been determined but this is probably dependent on the level of calcium channel blocker and its relative effect on these tissues. Generally, calcium chloride 10% with 10-20ml (10-30mg/kg in children) or alternatively calcium gluconate 10%, as 0.2-0.5ml/kg/dose up to 10ml/dose, administered by slow intravenous push over 5 to 10 minutes is the usual dose recommended. The dose may be repeated every 15 to 20 minutes depending on the clinical response. Administration of >45 mEq may lead to hypercalcemia. Patient should be monitored closely for development of cardiac arrhythmias.
| Controversies Over the Use of Calcium Channel Blockers |
|---|
| In a review entitled "Calcium antagonists: Overused and inadequately assessed" published in the June 1996 issue of Prescrire International (pp. 87-89), it was mentioned that a controversy opened up recently with the publication of studies casting doubt on the safety of nifedipine. The review based on a prospective search for clinical trials in cardiology over the last decade concluded that the clinical assessment of calcium antagonists is still inadequate. Available results challenge their preventive efficacy, as well as the safety of high-dose nifedipine. The reasons for these disappointing results are controversial.
It further adds that Americans experts of the National Heart, Lung and Blood Institute (NHLBI) declared that: "Short-acting nifedipine should be used with great caution (if at all), especially at higher doses, in the treatment of hypertension, angina and myocardial infarction. It is not yet clear whether the conclusions on short-acting nifedipine should be extended to other classes of calcium channel blockers or longer-acting dosage forms of nifedipine, or to other longer-acting dihydropyridines." Similarly as late as November 1995, the influential nationwide US consumer organization, Public Citizen, called on FDA "to require a warning on all calcium channel blocking drugs". It suggested that the labeling on all calcium channel blocking drugs is to include recent evidence linking these drugs to an increased risk for heart attack. It gave a summary of the following recent scientific evidence in support of its claim:
These studies consistently show a strong link between the use of the calcium channel blocking drug nifedipine and an increased risk of death and heart attack. Other calcium channel blocking drugs diltiazem, isradipine, verapamil have been implicated in increasing the risk of adverse cardiovascular effects in patients with high blood pressure or heart disease. This mounting evidence places in question the safety of other drugs in this class - amlodipine, bepridil, felodipine and nicardipine. It petitioned that the failure to warn doctors and patients of the potential serious effects of this class of drug when safer effective alternatives can be used as initial treatment for high blood pressure and chest pain will contribute to thousands of preventable drug-induced adverse effects annually, including deaths and heart attacks. |
Besides calcium, drugs that improve myocardial contractility such as isoprenaline, dopamine, adrenaline and noradrenaline have also been tried with varying degree of success. Glucagon has been used with some success in combination with calcium chloride and may be considered in calcium channel blocker overdose. It is said to be able to overcome the heart block and myocardial depression by increasing the production of cyclic AMP. In severe hypotension, the choice for the most appropriate drug can be guided by a placement of a Swan-Ganz catheter. Atropine have also been tried for the treatment of symptomatic bradyarrhythmias and the outcome has been discouraging. Generally, conduction deficits and bradyarrhythmias are not treated unless it contributes to the hypotension. Cardiac pacing is recommended in patients suffering from severe bradyarrhythmias. Enhanced elimination through means of dialysis and hemoperfusion are not effective in treating calcium channel blocker overdose since these drugs are highly protein bound.
4-Aminopyridine which is used in Europe to reverse the neuromuscular blockade induced by curariform drugs have been found to be able to oppose the effects of verapamil. It has been used in verapamil toxicity due to renal failure, reverting a third degree block to sinus rhythm. It works by blocking the the voltage-dependent potassium channels in excitable membranes, which indirectly increases the transmembrane calcium movement.
Two derivatives of dihydropyridine, Bay 8644 and RS30026 is currently undergoing studies to assess its potential as antidote for calcium channel blocker overdose. These two experimental drugs that have been shown to antagonise the blockade effects of calcium channels in both heart and blood vessels in animal studies by way of increasing the opening time and decreasing the closing time of calcium channels. It is believed that these drugs will soon be used clinically for the treatment of calcium channel blocker overdose.
