![]()
1995-1999: Five Years of Putting Information into Action
Inform@ction - The PRN way
For the last five years, one consistent effort made by PRN is to put informa tion into action. Being a national resource and information centre, the only one with respect to poisons and poisonings, the
trust is to 'inform' and, at the same time bring about 'action' towards greater public safety and health awareness.
With the dawning of the year 2000, as PRN celebrates the fifth anniversary of its establishment, inform@ction - the PRN way of putting information into action, has become its hallmark. From the outset the Centre has attempted a variety of inform@ction initiatives. It highlighted the dire consequences that some issues would cause if no action is taken.
In this context, PRN strives to proactively give the best available evidence and latest objective findings in support of its claim for action. At times it faces the risk of being challenged because it goes against the norm. But the Centre's tenacious position has helped by encouraging a free flow of information and not shying away from occasional public discourse and debate.
The Centre's bulletin is one such platform for discourse and debate. This issue of PRN8099 is the first in the new year, following some 25 others since 1995. It is published alternately with the Bahasa Malaysia sister bulletin, PenawaRacun targeted more to the members of the public. Together, more than 55 issues have been published to date featuring reviews of poisons and articulating current national issues. All copies of the bulletins are accessible from http://prn.usm.my/bulletin/index.html
Instilling awareness
Having a good rapport with the meida is an asset to PRN in its efforts to create and instill awareness on some of the issues affecting public health and safety. Since its inception, it has the privilege of working with three of the nation's mainstream newspaper by contributing weekly or biweekly columns on current health and safety issues.
More than 250 articles were published until the economic downturn hit the operations of many of the nation's newspapers. All of the columns provided excellent opportunities in dealing with urgent issues affecting the public at large.
Despite the difficulty, the ‘Poison Control’ column started in the New Straits Times remained intact. Although it was changed into a 3- weekly column as the economic pressure mounted, but beginning November 1999, it was reinstated as a weekly column. In fact it has now found home in the Sunday edition of the newspaper as part of the paper’s Science page.
To date close to 400 articles were produced, including a series of topics in a popular science and technology magazine. It covered issues ranging from the dumping of cyanide in the country's resort
area to the world's worst haze blanketing the region; from a national lead scare in some branded colouring materials to dioxin-tainted in food; from drug and tobacco dependence to the rational
use of medicines. These are clear examples of when information were put into action providing the public with feedback as to what they could do to enhance their own health and safety.
To supplement its effort in running a column relevant to current national interest, PRN initiated a bold step of clipping news items from 5 national newspapers (3 in English, 2 in Bahasa Malaysia) daily. This is to have a feel of what are issues of concern on the ground that must be focused on with respect to health and safety issues in general. Over time the clippings have in themselves turned to be a very useful reference source to PRN of more than 10,000 entries on various topics covering the period 1995-1999.
A special computerised retrieval system to develop to document and retrieve these news items. In attempting to pass some of the benefits to members of the public, Malaysians in particular, a good number of them were summarised and placed at PRN’s website (http://prn.usm.my) on a regular basis. Many, mainly among students in schools and institutes of higher learning, gained from such a resource in the effort to retrieve local information on a particular aspects. Presenting these incidences in the form of a global diary, ‘The Poisoned World’ was created. It provided an indication of what were the important events happening in the different parts of the global at different periods of time.
Your gateway to information
The inform@ction strategy took to the cyberspace in 1996 when the Malaysian Drug and Poison Net was launched in April 1996. Also known as ‘prnnet’ it became PRN's homepage meant to document over the Internet the major activities as well as services it has been offering. A specific mission statement was created for this, namely: ‘to promote health in an information society, and to provide information for a healthy society’.
This mission statement lent more room for the homepage to expand. In the next three year, a number of websites were launched especially as part of its advocacy role. Examples are websites on tobacco (United for a tobacco-free Malaysia), Viagra (ViagrAlert), Nuclear Disarmament (Hiroshima on my mind), essential drugs (Essential drugs in Malaysia), and more recently on lead poisoning (Malaysian Resource and Information on Lead). From time to time, PRN put up ‘Current Issue’ website, the latest on Y2K and Health. Others were on fluoride/fluoridation, dioxin, arsenic, and the haze to supplement public informational needs from time to time.
With all these development more information are being put into action. Hence there is a need to re-create and re-launch the original ‘prnnet’ website. This was done in 1998 with the renaming of the new website as ‘prnweb - your information gateway’ - an enlarged version of ‘prnnet’. The prnweb has also taken an international dimension by hosting a number of websites belonging to international initiatives like International Society of Drug Bulletins (ISDB) and International Network of Drug Information Centres (INDICES), and also special local interest group website spearheaded by the Citizen's Health Initiatives.
Under the ‘prnweb’ too, a News & Health Information section has been upgraded as a main website on its own right. It documented not only the thousands of summaries of news clippings, but also included under the section are specialised news topics related to drugs (Drug News), tobacco (Tobacco News), Viagra (Viagra News) and recently on lead (Lead News). All the specialised sub-topics are intended to keep track of the advocacy role of the Centre. They serve as barometers to inform@ction.
Some inroads
In short for the last five years, PRN has successfully put information at its disposal into action in meeting its mission ‘to reduce mortality, morbidity, occurrence and cost of poisoning in a manner that
strives for excellence, compassion and innovation’.
In year 2000, inform@ction gained momentum, when the Ministry of Health planned to introduce a National Surveillance Programme on Lead Poisoning. Based on research undertaken in several states since 1996, PRN has been a proponent in promoting this initiative. Other achievements that could be accorded to inform@ction were the labelling of all fluoridated toothpastes produced in the
country, and the banning of the use of laser in toys. The directive to label all fluoridated toothpaste manufactured in Malaysia was issued by the Drug Control Authority in 1998. The need for this was
highlighted with the aim to further protect the health and safety of children below the age of 6. Similarly in the case for the banning of the use of specific class of lasers in toys beginning in 1999.
PRN with support of many, especially the Sekolah Menengah Seberang Jaya, has managed to sustain a school-based smoking -- Kelab Nafas Baru -- the first of its kind nationally. This initiative is being emulated by many other schools.
More recently the introduction of the National Drug List for both the public and private sectors has also received wholehearted support from PRN since it was first proposed in 1996. The Centre has
always advocated the judious and rational use of drugs, earning it the designation as a WHO Collaborating Centre for Drug Information in 1998 - the first in the region. The Collaborating Centre since
then has established two Information Exchange Network covering the Asia-Pacific region on matters relating to pharmaceuticals, biological and herbal medicines.
In the years to come, inform@ction will continue to be the hallmark of PRN drives for a better and safer place to live. This is in the tandem with the move towards a more knowledge-orientation society
where information is the driving force. Since information is the basis for creation of new knowledge, it follows that the former must be driven into action to produce the desired knowledge required for
a safer and healthier life.

For the year 1999, PRN undertook two studies as part of its long-term commitment on lead exposure among pre-school children. The first was in Sabah, an on-going collaborative project undertaken together with Yayasan Sabah; and the other is a new initiative taken in Johor supported by the State Government. Below are the study briefs.
Follow-up project on lead exposure in Sabah (Phase III)
The objective of the project is to study the extent of lead exposure in the pre-school children in the west coast of Sabah and its effect on their IQ.
This is a follow-up study from the previous two studies which were carried out in 1996 and 1997 respectively. The study was supposed to be carried out in 1998, but it was postponed due to the prevailing economic situations. In the first two studies, it is evident that there were a number of children from the west coast areas of Sabah who experienced high blood lead. Although majority of the levels are not considered critical, some of them that needed constant monitoring. A trend among the siblings of affected children also showed certain level of lead exposure in them. One implication of this finding is that they were subjected to a continuous lead exposure. From the results of previous studies, it is apparent that lead accumulation occurred in some of the children. The source of exposure has yet to be determined and identified.
The 1999 study looked at the following:
- to monitor and identify the level of lead exposure among those children that have been identified in the previous study to possess blood lead level of 5.0 mcg/100ml and above,
- to identify possible sources of lead exposure, and
- to find any relationship between lead exposure and IQ.
Sample populations from two districts were identified to participate in this follow-up study. Thirty-six pupils were selected based on the previous study results. Only those with blood lead concentration of 5.0 mcg/100ml and above were chosen. Blood samples were obtained and analysed by graphite furnace atomic absorption spectroscopy (GFAAS) as done previously. A number
of environmental samples such as soil and water were also collected and analysed.
In addition, the students were asked to take an IQ test using the modified and validated version of McCarthy Scales of Children’s Abilities. All sampling and tests were carried out with a written approval from parents. The study was funded by Yayasan Sabah. The completed report will be submitted to Yayasan Sabah and is the final stage of analysis.
Project on lead exposure in pre-school children in Johor (1999 – 2000)
The project initiated in 1999 had the following objectives:
- to identify and monitor the level of lead exposure in preschool children in the district of Johor Bahru,
- to identify the high risk areas, and
- to identify the population of children affected by high lead exposure.
The sample population for the study was obtained from 230 registered public and private kindergartens in the district of Johor Bahru. The students were randomly selected from the list of pre-school children in the respective kindergartens.
A total of 500 pre-schoolers were randomly selected and screened for lead exposure.
In order to facilitate their participation in the study, special briefings were held for parents and schools teachers whose children and school were selected for the study. During each briefing,
participants were presented with a video on lead followed by lecture and question/answer session. This include topics on the sources of lead, common items and household products thay may
contain lead, and how to prevent lead poisoning. This two-pronged strategy helps to create public awareness about lead in environment as well as the risk of lead poisoning.
The study is part of a larger study funded by the State of Johor through its community-based subsidary Yayasan Pembangunan Keluarga Darul Takzim. The first part of the study has been completed where 230 blood samples were collected and analysed. The outcome of the study will be submitted to the Johor State Government for further consideration.
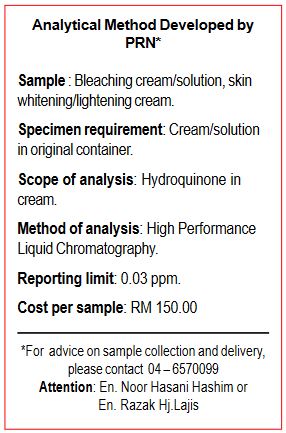
Analysis of Hydroquinone
General
Physical and chemical properties
and quinone.
Melting point: 173 – 174oC
Boiling point: 287oC
Solubility in water: 70 g/litre at 25oC
Uses
Hydroquinone is extensively used as reducing agent, photographic developer, stabiliser or polymerising inhibitor for certain materials that polymerise in the presence of free radicals, and as a chemical intermediate for the production of antioxidants, antiozonants, agrochemical, and polymers. It is a skin-lightening agent and is used in cosmetics, hair dyes, and medical preparations.
Clinical and toxic effects
Hydroquinone is rapidly and extensively absorbed from the gut and trachea of animal. Absorption via the skin is slower but may be more rapid with vehicle such as alcohols. Hydroquinone distributes rapidly and widely among tissues. Death has occurred from the ingestion of as little as 5 grams. Ingestion of as little as one gram has caused nausea, vomiting, ringing in the ears, delirium, a sense of
suffocation and collapse. Industrial workers exposed to the chemical have suffered clouding of the eye lens. Application to the skin may cause allergic reactions. There are case reports that skin lightening creams containing 2% hydroquinone have produced leukoderma as well as ochronosis. Hydroquinone (1% aqueous solution or 5% cream) has caused irritation (erythema or staining).
PRN CONSULT
In conjunction of the National Surveillance Programme on Lead Poisoning Workshop, 20-24 February 2000, Penang
Review on
Lead Poisoning
by Rahmat Awang PharmD
Introduction
Lead is the most common cause of poisoning involving heavy metals. Most lead poisoning however is slow in on-set and as a result of long-term exposure and gradual accumulation. Acute lead poisoning, though rare, has occurred in a limited number of cases. In adults, this has been confined to high-dose inhalational exposure associated with the use of a heating gun, acetylene torching of lead and repeated inhalation of organic lead such as petrol. In children it is often associated with repeated ingestion of house dust or paint chips containing lead salts. This article intends to review the problems seen in lead poisoning and how they are usually managed.
Are all forms of lead toxic?
Lead is available in many forms. The elemental lead which is the metallic form of lead is not well absorbed when ingested. This does not mean that it is not dangerous because the extent of its ab-sorption can be improved if it is converted to vapour by the process of heating the lead. Lead salts on the other hand are better absorbed. Most products contain lead salts but fortunately the amount is relatively small to cause acute lead poisoning. Despite the small amount, poisoning can still occur with lead salts but ,this is usually due to long-term exposure. The other form of lead is the organic lead compounds. Tetraethyl lead is one form of organic lead. It is found in gasoline which is well absorbed through both the inhalation as well as the oral routes.
There are a number of incidences where ingestion of several grammes of lead acetate or tetraethyl lead or from lead curtain or fishing weights that had remained in the gastrointestinal tract for a number of days cause poisoning. Lead is likely to accumulate in the body to cause toxicity when more than 0.5 mg/day is absorbed for several day.
What are the effects of lead poisoning?
Ingestion of a very large amount of lead within a short period of time may result in the patient to experience abdominal pain, vomiting and diarrhoea. Repeated intentional inhalation of leaded gasoline has been noted to cause ataxia, myoclonic jerking, delirium and convulsions. Chronic exposure leading to intoxication may cause abdominal colic, constipation, anorexia, headache, irritability, fatigue and anemia (macrocytic more common than microcytic). In addition to this, patient may suffer from peripheral motor neuropathy manifested in the form of wrist or foot drop. Encephalopathy in association with cerebral edema has also been reported and this seems to occur more commonly in children. It is characterised by ataxia, delirium, depressed consciousness, coma and seizures which represents a life-threatening emergency.
The nervous system involvement is more predominant in adult than in children. This may be manifested in the form of fatigue, irritability, lethargy, insomnia, headache, difficulty in concentrating, memory loss, and tremor. In addition to these, patients may suffer from myalgias, vomiting, constipation and loss of libido.
At a level of more than 150mcg/dL, life-threatening neurotoxicity may develop. Other CNS effects include marked disturbances in auditory brain stem evoked potentials.
What are the pathophysiologic effects of lead?
There are a number of areas where lead can exert its effect. At the cellular level, lead reacts with the sulphuhydryl groups and interferes with enzymes that are involved in the heme synthesis (see
Figure 1). As a result, there is interference in the production of hemoglobin and cytochrome.
Lead too interferes with the action of aminolevulinic acid (ALA) dehydratase and coprophyrinogen decarboxylase. This will block the conversion of delta-aminolevulinic acid to porphobilinogen and coproporphyrinogen III to protoporphyrin IX. Consequently, ALA and coproporphyrin accumulate in the urine. The elevated levels of ALA and coprophyrinogen have been used as biochemical indicators for lead poisoning. However, these levels are also elevated in patients with hereditary copropor-phyria and variegate porphyria. Thus, the blood lead level needs to be determined in order to differentiate between the prophyrias and lead poisoning. In addition to this, lead also blocks ALA synthetase and ferrochelatase leading to the accumulation of protoporphyrin in the red blood cells.
Lead can interfere with the sodium-potassium ATPase pump mechanism. In blood, lead attaches itself to the membranes of the red cells making them fragile. This resulted in a decreased survival of the RBC. Lead also has an affinity for hemoglobin thereby interfering with heme synthesis. This finally resulted in anemia In an attempt to compensate for the resultant anemia, the bone marrow responded by increasing the production of RBC and releasing immature RBC. Examination of the blood shows the presence of reticulocytes and basophilic stippled cells that represent abnormally
aggregated ribosomes.
Lead poisoning may affect the kidney, the heart and the nervous system. The effect on the kidney is such that acute poisoning cause a Fanconi-like syndrome, whereas chronic poisoning caused chronic nephritis. Lead can also cause swelling of the heart fibres leading to myocarditis and eventual fibrosis.
On the brain, lead has been reported to cause cerebral edema. It has a direct cytotoxic effect and the ability to penetrate neurons at low levels to interfere with neuronal metabolism. In this re
spect, the gamma-aminobutyric acid (GABA)-mediated inhibitory pathways become affected. This is thought to be the cause of behavioural changes seen in children exposed to lead. Peripheral neuropathy is another problem seen due to the effect of lead on the myelin sheath. The effects on the central nervous system are often irreversible. About 85% of those who develop encephalopathy may suffer from permanent brain damage. Additionally, decreased nerve conduction, lower IQ’s, increased psychomotor activity, and learning disorders have also been reported in children with blood lead that is below the “toxic” level. Despite this, there is still much debate about the effects of chronic exposure to subclinical doses of lead.
Lead crosses the placenta and has been shown to affect fetuses. High lead content in pregnant women may contribute to increased fetal wastage while high lead content in the placenta and fetal membranes has been associated with premature rupture of membranes and preterm delivery. Spermatotoxic effects on the male also exist, manifesting as infertility. The toxic effects on human reproduction however are not well elucidated.
How does one diagnose lead poisoning?
Lead poisoning is known to cause an array of medically-related problems. The signs and symptoms manifested, espe-cially in chronic poisoning, may be non-specific covering a number of organ systems Poliomyelitis, diptheria, polyneuritis and porphyria (in children that is en-tering into puberty), all presents in a manner similar to chronic lead poisoning thus making diagnosis a challenge
A good history that relates to potential exposure is often required to direct doctor to suspect lead poisoning. Patient with history of potential exposure and suffering from conditions such as microcytic anemia, abdominal complaints, or neuropathy; or any child with delirium or convulsions should be investigated for possible lead poisoning.
In acute poisoning, the patient may present with anorexia, constipation, abdominal pain, behaviour changes, vomiting, lethargy, hyperactivity, clumsiness, ataxia, convulsions, and coma.
If lead poisoning is suspected, a number of laboratory tests should be ordered. The laboratory results may reveal increased urinary coproporphyrins, blood lead levels greater than 60mcg/ dL, erythrocyte protophyrin greater than 190mg/dl or 7-10 times higher than normal.
In chronic lead poisoning, the signs and symptoms are generally non-specific. It may range from vague aches and pains, wrist and ankle drop to chronic nephritis. X-rays of the abdomen section may reveal radiopaque flecks of paint, while x-ray of the long bones may show presence of lead lines indicating premature opacification of distal long bones in children.
Laboratory tests performed may reveal haemoglobin level of less than 10mcg/ dL, basophilic stippling, increased urinary ALA, blood lead levels of 30-60mcg/dL. If anemia is present, it should be distinguished from iron deficiency anemia. The presence of an elevated rather than a lowered reticulocyte count in a child with suspected ingestion gives a strong indication that the anemia is due to lead poisoning, rather than from iron deficiency. However, it must be remembered that patients who are at greatest risk of lead poisoning are often malnourished and suffers from iron deficiency anemia.
What are some of the methods of testing for lead poisoning?
There are a number of tests that are carried out in cases of lead poisoning. The most reliable test is the blood lead level itself and this is well suited for mass screening. Another test that is being employed is the EDTA mobilization test. This test measures the total body burden of lead, providing an evaluation of chelatable lead stores. The test is done by administering 20-25 mg/kg (500mg/m2) EDTA in 100mL of dextrose 5% by intravenous infusion over 1 hour, followed immediately by an 8 hour urine collection. By measuring the amount of lead (in mcg) excreted in the urine and dividing it by the amount of EDTA given (in mg) gives a lead extraction ratio. A value of 0.6 is interpreted as positive and provided an indication for chelation therapy.
Another test that is carried out is the free erythrocyte protoporphyrin (FEP) or zinc protoporphyrin (ZPP) tests. The test provides an indicator of lead-induced inhibition of heme synthesis. The test is sensitive enough to be employed for screening chronic exposure.
